I’ve been reflecting on this nugget over the past 12 months, and it’s definitely worth re-visiting. In our current times, the messaging that our elderly population is at risk and vulnerable is loud and clear. While this may be necessary from a risk perspective, I ask myself might it also be an opportunity to remind older people of their strengths, their wisdom, and dispel the ageism myth which is often a big, fat DIM?
This ‘Crisitunity‘ can be a great chance to remind your patients, your loved ones and your wise friends that walking and moving can be really powerful SIMs which can, while still being COVID cautious, help strengthen the immune system and enhance quality of life.
Case Study: ‘Joyce’
It’s always important to listen to current information and it is equally important to put that information into perspective in order to understand the whole story.
Joyce, my 89-year-old ‘American mum/mom’ lives alone in her beach shack in Long Island New York. She is a very social human and an active member of the Democratic Party in her community. As an election year, 2020 promised to be a busy one for Joyce out in the community but when COVID hit, she found herself increasingly isolated from her family, her friends and her community.
Active her whole life, exercise and movement is as important to Joyce as eating and drinking. She also loves a glass of wine or three and won’t say no to a cocktail any day of the week.
With a forced lockdown and family staying away, Joyce noticed quickly that her mobility was reduced, the lockdown acting as a magnifying glass to her self-image as an aging person confronting her mortality. She generally wasn’t feeling well. It’s not easy for a 90-year-old to wear a mask. She’s not used to it. Wearing a mask was uncomfortable and she felt it ‘threw her balance off’. Joyce has style, she pays attention to putting herself together and styling it up even on a trip to the grocery store. Her confidence was waning and she started to feel like she may never be able to do the things that she enjoys again. Given my field of work involving contact with many people, her family initially asked me to stay away. Joyce was conflicted, wanting social contact and at the same time not wanting to jeopardize her health. She was nervous and questioned her ability to walk even the short walk to the beach, which was previously little to no effort for her.
Given that I lived fairly close to Joyce I’d ring before doing my shopping and would often drop off food and basics as Joyce was not comfortable leaving the house. Joyce was very grateful. She has always been fiercely independent and didn’t want to be a burden. After a few weeks and my first negative COVID test, I could tell Joyce was anxious to take a walk and she agreed to a socially distanced walk. We wore a mask and did her usual walk.
After the first few minutes, Joyce was clearly uncomfortable with her mask. I invited her to remove it – there was no-one around and we were adequately distanced. She walked with greater confidence. I asked her how she was feeling, she said she loved being able to walk again. ‘I guess I’d better get used to the mask’ she muttered, so we tried it again. I asked her to focus on an object in front and look toward it, counting the steps and focus on ‘feeling her feet on the ground’. It can be difficult to be kinesthetically aware of all your body parts and follow instruction, however, Joyce focused on ‘foot/eye co-ordination’, feeling her feet touch the ground. Keeping the chin up was another cue that could facilitate this process.
On that first day, Joyce walked further than I would’ve thought, showing no signs of fatigue: to the contrary, she was noticing her surroundings and commenting on the thoughtlessness of her neighbors for putting a mirror on the outside of their garage, confusing and a possible danger to the native birds which she deeply cared about.
With each step, Joyce’s confidence improved and she was able to make it around the block, then back to the beach. As she looked out at the ocean which she loved, her eyes opened and for a moment she was out of lockdown and opened up. Suddenly she articulated what really bothered her: confronting her own mortality. And then reassuring herself that she could cope with it.
It was a challenging summer for Joyce, eventually her daughter came out to stay with her, and she did fall once while wearing her mask in the supermarket. That wound took a long time to heal and again her walking suffered. The next big step was going out for the first time. It was her daughter’s birthday and being summer, we were able to sit outside and enjoy a lovely celebration. Joyce’s spirit immediately lifted.
The wound on her leg continued to take its time to heal. She had many trips to the hospital and was put on various medications, one interfering with her gut. One night her iron levels dropped, almost causing sepsis.
From October to December Joyce continued to improve. Months later, I was back in quarantine after contracting COVID from a patient, and it was Joyce who came to me to drop off food. It was very gratifying and it made me stop to reflect that it’s not just our age and whether or not we have co-existing conditions, it is our attitude and support network that determines how vulnerable we really are.
–Luke Bongiorno
Explain Pain Supercharged, Novella #11: Oldies are goldies
We are all living longer – 60 is the new 40, 80 is the new 60…? This is usually a good thing but ageism is in the air. Ageism is a negative perception of getting older and of older people. It’s a really big DIM and it needs to be challenged. Young and old people can be ageist, older people can be ageist about themselves. Health professionals and sometimes government departments and companies can be ageist. Let’s challenge it, first by obliterating some myths about pain and ageing.
Myths about pain and ageing
Myth 1: Pain is inevitable with ageing.
This is not true, but most people including some health professionals think it is. Sure, there may be a few more illnesses and surgical procedures but people over 60 have no more migraines, no more back pain, no more neck pain than younger people have. In fact, the oldies may have less pain.
Myth 2: If you have some pain now, then you will have worse pain later.
This is not true either. Pain comes and goes in older people just like it does in younger people. Even though x-rays and scans may show things such as narrowing of joint spaces, this has no relation to increased pain. These are age changes and more age does not equal more pain. Rest easy…
Myth 3: Toughing it out makes it easier to tolerate.
Some of us oldies think ‘I can grin and bear it!’ This might be true for a while, but we know that it doesn’t make anything easier in the long run and being stoic can lead to depression, which in turn increases pain more in oldies than it does in youngies. You don’t have to ‘grin and bear it’, ‘suck it up’ or accept it as part of ageing – seek help from an up to date health professional, just as you would if you were younger.
Myth 4: There is nothing you can do for it.
This is rubbish! There are treatments that work for youngies, middlies, oldies and ultra-oldies, such as Explain Pain combined with contextual activity exposure. The Protectometer approach is ideal for oldies alongside appropriate medications.
Age is only a number, it is not an excuse.
The protective power of SIMs
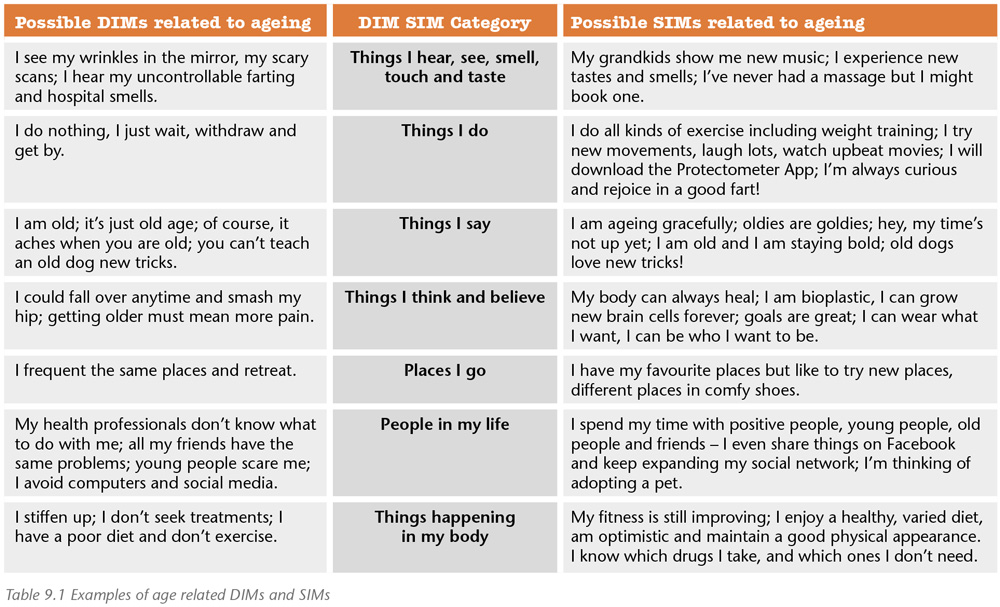
Here is a really important study – we know that people who have a positive self-perception of ageing when they are 50 will live on average 7.5 years longer than those who have a negative self-perception of ageing at 50 [5]. Of course, many things will influence self-perception. Positive self-perceptions are SIMs. Table 9.1 (above) shows a list of SIMs and DIMs related to ageing. This list was first put together for an elderly and ageist patient who declared that she was ‘ready for the scrapheap’.
A few more good things about growing older
Let’s stop for a moment to remember the good things about getting older. You don’t sweat as much as those smellier youngsters, if you’re bald you can avoid hairdressers (imagine the money you save on shampoo), you can easily see the good and ignore the bad, you problem-solve better than youngies because your brain has more efficient connections, you want less and you have fewer allergies.
Ponder this
Next time you are talking about your sore knee and someone, perhaps it is your health professional, says ‘It’s just old age’ or you think that yourself, then ask them (or yourself) ‘is my right knee older than the rest of me?’
Linked Target Concepts
Pain and tissue damage rarely relate (3)
Learning about pain can help the individual and society (9)
Active treatment strategies promote recovery (10)
Additional resources
Related ‘jams:
The challenge of surgical masks for physiotherapists
comments