The Protectometer has to be one of the most useful clinical tools which has arrived on the scene in decades, and is now at our disposal. From the days when James Cyriax proposed ‘Extrasegmental Innervation’, back in the nineteen fifties, to today’s understanding of peripheral and central sensitisation, we have come a long way in my clinical lifetime. The Protectometer now enables us, the clinician and the patient, in a very simple way, to bring sense and meaning to the sometimes supposedly bizarre array of experiences that patients and clinicians witness. Below is a very simplified case history to demonstrate my enthusiasm about our new and, for me, now invaluable addition to our repertoire.
A poor prognosis
Mrs Delightful Lady (Mrs DL) suffered leukaemia some eighteen years ago. She was taken to the very edges of death through the chemotherapy, and bone marrow transplants. During her treatment Mrs DL also endured multiple lumbar punctures, one of which added a ‘right foot drop’ to her ordeal. Mrs DL was warned that her prognosis was indeed very poor. Additionally, her psychosocial realms, both personal and interpersonal, were on full stretch from all sides.
Mrs DL survived and leads a full life with husband and children, however the ‘sometimes 12/10, constant burning pain from the knees down’ makes life a great challenge. Additional pain experiences of other body parts have joined the leagues of misery. The present diagnosis is ‘peripheral neuropathy’. The current medical team have suggested that nothing can be done other than to ‘manage‘ the pain with ever increasing amounts of medication. This approach is delivering ever decreasing amounts of relief. In her mid-forties Mrs DL wonders were this will all end and how much longer she can endure the prognoses of the future. Mrs DL is a fighter and of course she will soldier on but at what price to all concerned.
Sceptical at first
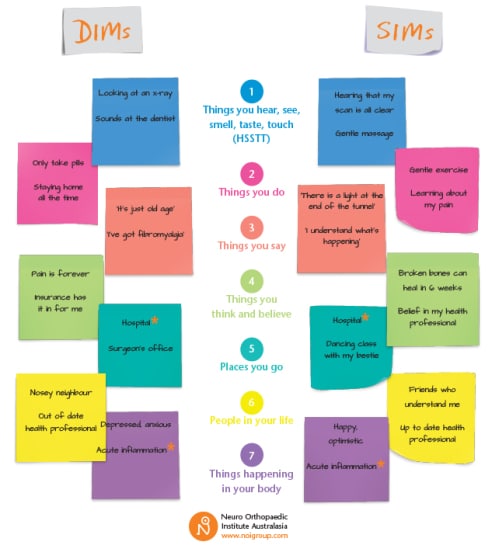
We added the Protectometer handbook to our clinical journey and Mrs DL was sceptical at first but by now was slowly buying into our Explain Pain Journey. As usual, identifying the more psychosocial DIMs is always a challenge. Whilst chatting one day I mentioned the Royal Free Hospital and immediately felt an emotional response from Mrs DL. Apparently the Royal Free was where she had had her bone marrow transplant and had been informed, just before the treatment, that this was her last chance and the prognosis for a good outcome was a mere twenty percent (DIMs?).
A conscious sharing
This conscious sharing of a very negative experience (a powerful DIM), and the emergence of similar experiences hailed an improvement on the meter scale. The ‘bath water’ level sank.
In a clumsy moment, at our last meeting, when going through her meter I said ‘7/10… that bad!’ to which she replied, ‘no, that good!’
A combined front
Feeling out of my depth on the PS front I suggested a visit to our psychotherapist team member to explore her ‘demons’. On this combined front I believe we will build even greater inroads into her pain experience. I very much doubt that those demons would have surfaced in front of a physiotherapist without the use of this vital tool, the Protectometer. And I very much doubt that Mrs DL would reflect on entering into psychotherapy without the trust she had in her physiotherapist.
3 October 2015
Sardinia 😎🍷🍝
David Bolton, MCSP MMACP MSOM, has over 40 years of clinical experience in the field of neuromusculoskeletal medicine and is a long time NOI faculty member. After qualifying in 1971 from the Royal Army Medical Corps School of Physiotherapy, David spent 24 years living and working in Switzerland, running a busy and very successful private practice as well as providing specialist physiotherapy services to the Swiss Alpine Downhill Ski and Ski Jumping Teams, the Swiss National Karate Squad and the Menuhin School of Music.
In 1997 David decided to down size and move his practice back to his roots in London. Setting up Limbus in Chelsea Harbour, David now specialises purely in acute and chronic, therapy-resistant pathologies, biopsychosocial thinking being the core of his treatment philosophy.
In his free time, when you can get him off the tennis court, David loves to travel.
Great work David. Good case study. JohnB
Hi David,
Thanks for this. I must admit that some years ago, hearing such a history may have turned me into a DIM as my body language “said” what on earth can I do here?” There are many missed groups out there who deserve the dignity of an explanation. I would love to hear how she progresses.
By the way, I would also assess and if appropriate, wriggle and jiggle her neuromeningeal tract as part of graded movement. Sometimes those lumbar punctures pop a vein and blood of course is rather glue like!
Thanks
David
Hi David,
Yes there are no boundaries limiting who can profit from the protectometer. I’m using it with a patient who’s case history is only eleven weeks old at the moment.
I totally agree with you on the meningeal question. Being a very hands on therapist I am “All over” her Nervous system. Naturally, in addition to the “Knowledge” I am adamant that a hands on component is always a vital part of treatment even if it is limited to a big hug.
DB
London ☔️