It’s hard work achieving deep and durable conceptual change and clinically important behavioural change with Explain Pain – it takes time, rebuffs are common, health practitioners rarely have teaching experience and consequently much ‘Explain Pain Light’ is carried out in the world.
One of the key skills when Explaining Pain is to identify the essential curriculum Target Concepts appropriate for an educational intervention for a specific person or group. An example of a frequently used Target Concept may be: Pain relies on context. Once the learner understands the concept, with some help, it can open up a vast store of functional knowledge, for example an understanding of why it hurts more in environments perceived to be dangerous.
Lorimer Moseley and I have extracted ten key Target Concepts for the upcoming Explain Pain Supercharged (Moseley & Butler 2017). In a group setting, where time allows us to dive deep into pain biology, we would use all ten of the Target Concepts to construct a detailed curriculum. Similarly, a curriculum for an individual with a long standing and complex pain state would also cover all ten. But a shorter intervention for an individual with a less complex pain state, or for a group presentation with the goal of giving the participants just a taste of Explain Pain, would see fewer Target Concepts addressed, perhaps with some merging occurring too.
Here they are…
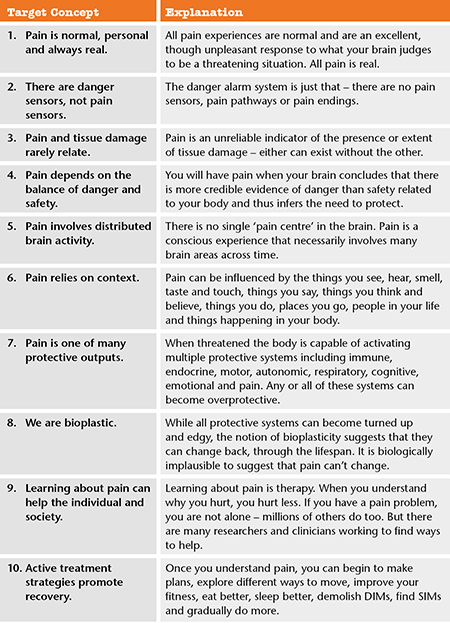
We think this list of Target Concepts is quite novel, and represents the first time they have been extracted, explained and made ready for inclusion in a comprehensive Explain Pain curriculum. And we think that if nothing else, considering these Target Concepts in every Explain Pain educational intervention will help to improve outcomes – in the clinic and the research lab.
What do you think? Have we covered everything? Would you word them differently? Thoughts and comments welcome below.
– David Butler
Explain Pain Supercharged – an update
Explain Pain Supercharged, from Lorimer Moseley and David Butler, is full of brand new content and will Supercharge your Explain Pain interventions in two essential ways:
- Over the years, you’ve asked for it, and we’ve delivered – we’ve gone deep on the neuroimmune biology of pain with comprehensive sections detailing the latest from pain science research and its application to the clinic
- For the first time, educational science, conceptual change theory, metaphor use and curriculum development has been brought together specifically for health professionals delivering Explain Pain. 71 Neuroscience Nuggets, 15 Novellas and 4 comprehensive, targeted Explain Pain curricula have been provided, along with the framework to implement them into any treatment program.
Explain Pain Supercharged is at the printers and we’re expecting the truck any day – we’ll let you know as soon as sales go live.
Beautiful, says it all, I feel 25 years of personal study has been paraphrased perfectly ….for me personally all ten points are always relevant at all times In all situations.
Thanks David,
Even in situations where I may have, say 5 target concepts, elements of the others would probably be absorbed.
All the very best
David
Pain is also about behavior, the sufferer may show protective behavior, fellow humans may show empathic behavior and ultimately group behavior may tend towards cooperation.
Of course there’s also maladaptive behavior.
Hi Marcel,
I think we have encapsulated this in the target concepts or at least made them liberal enough to.
I don’t use the term ‘maladaptive’ much these days – everything is adaptive. I am always wary of a judgement of ‘maladaptive’
Cheers
David
I love this, David. It’s all adaptive. You’ve been such a find for me this year — I’m an OT tech but I am trying to share your insights with every provider all around me as well as introducing these concepts to my clients. Thanks for your passion!
This is so helpful. Thanks to the NOI team for this. As a full-time clinician, it is difficult to find the time to sit down and think through these concepts and come up with a cohesive plan as to how I will educate the patient. Taking the step from “I need to better educate the patient” to actually, effectively educating the patient is a big one. Simply have a starting point is very helpful.
Hi Mike,
Thanks – and that is what it is – a starting point. Once the target concepts are established we will all have different stories, examples and tools to address the target concept. They are broad and we also have lists of different ways of expressing the target concept so that we can all (clients too) embrace them. (I will post some of these a bit later)
All the best
David
Unfortunately I admit that this is the weakest area of my clinical practice. I look forward to getting this comprehensive text on the latest knowledge about pain science. I’m hoping mine will be warm from the printing press. God Bless!
Hi Bruce,
I don’t think you are alone there! I think it is the weakest part of many clinicians’ interventions, including myself. We are not trained in education. I took five years off to do an education degree and I was embarrassed by how much I didn’t know in comparison to how much I thought I knew!
Good on you
David
Hello David, you asked for comments about the Target Concepts and Explanations. About Concept #6, Pain relies on context. It seems to me that memories and emotions ought to be included in the explanations. Such powerful factors. Perhaps you consider them to be included under other words in the explanation. Can you elaborate please?
Hi Johanna,
Thanks for this. The role of memories and emotions would be an important part of any Explain Pain intervention. On reflection, memories and emotions would be picked up in Target Concepts 4, 5, 6 and 7. In the case of 7 (pain is one of many protective outputs), emotions such as ‘the blues’ which initially could be seen as protective if they allow appropriate withdrawal and energy conservation, clearly can become potent contributors.
Lorimer and I have also listed ‘different ways of expressing the target concept’ to hep people embrace them and to realise they are very broad and liberal. For example Target Concept 5 ‘pain involves distributed brain activity’ could also be expressed as ‘pain can be modified by anything.’
Does this help?
Best wishes
David
David, in contradistinction to the Decalogue handed down on Mount Sinai, I note that you welcome comments. For the record, elsewhere in cyberspace I have posted this comment: “I am not sure I can agree with Points 1,7,9. Point 8 is clumsy. Point 10 is a motherhood statement.” Some of us are eagerly awaiting a revision!
Hi John,
You will have to eagerly await a second edition when we see how these stand the test of time. With many others, we have argued over the Target Concepts for a long time now, continually tested them at the clinical battlefront and are now fitting and testing them in questionnaires. We tried to make them short and punchy and as I have mentioned in other comments above, Lorimer and I have offered alternative ways of expression of the Target Concepts which may make them easier to engage.
1,7,9 are essential to our current explanations, 7 is sometimes difficult for medical professionals (perhaps a disadvantage of specialisation). I see no motherhood in 10, much more a critical Target Concept to challenge the passivity (read motherhood/fatherhood) which still broadly dominates health.
Nor should there be any motherhood(not really sure what that is) in learning strategies which aim to turn the Target Concept into functional knowledge.
Cheers
David
David, thanks for your response. I hope my concerns can be addressed in the next version of your Decalogue. I capitalised the term as many Health Professionals regard your pronouncements as being authoritative, whereas I am sure that neither you nor Lorimer have ever seen yourselves in this light.
Thank you for this David. It lays it out nicely and concisely!
I have been mulling over point 1 “ALL pain experiences are normal…” I am not comfortable with the word ALL in this point. Whereas all pain experiences are a result of the brain perceiving there is more danger than safety and pain is indeed a normal part of life, in conditions where there is ongoing pain or widespread pain, I’m not comfortable describing this experience as ‘normal’. I’m more comfortable describing it as a normal process that has become over sensitive so is no longer working to protect appropriately. There comes a point were processes cross the line between appropriate protection and over protection and I wouldn’t describe this over protection as ‘normal’. Would welcome your thoughts on this.
I also think it is worth highlighting the importance of ongoing support and the need to factor this into your curriculum. Very few do. Learning about pain is just the starting point. It’s a longer (lifetime) journey that takes a lot of courage, persistence and patience to stick at it. I believe people need ongoing support to stay on this path as it is easy to get side tracked off if you’re going it alone. Also to continue to progress they need to continue learning, evolving and adapting to new knowledge and changes in their individual circumstances. Clinicians need to offer this support in a way that doesn’t encourage dependency but in a way that enables growth and curiosity which isn’t easy!
So for me, building in some means of ongoing support into a curriculum is really important and, in my view, worth highlighting as a point of importance.
Hi Betsan,
Good points. It took me a while to internally endorse that “all pain is normal”, ie normal at all sensitivity levels. It wasn’t easy and I admit to occasional uneasiness. What is not ‘normal’ perhaps are the circumstances a person finds themselves in, perhaps picked up in Target Concepts 4, 5 and 6. So when a person is telling me the long , unpleasant and sometimes complex pain story that we have all heard, I can reflect ‘well with all that going on, it would be quite normal to have pain, in fact you would be quite abnormal if you didn’t have pain’. I find this quite liberating. There is a challenge to this of course with the ‘pain as a disease’ movement and the unease in horror situations which must involve significant neuroimmune rearrangement (this could be a blog post on its own).
Some thoughts: Ongoing learning/support should fit under Target Concept 9 though perhaps we need to express that more clearly. To be resource efficient, ongoing support may be access to and awareness of resources and not face to face. If Explain Pain is effective it should be more than just the starting point, it should provide durable conceptual changes which can be adapted to what life throws up, ie a self support system.
If you had a group, and particularly groups such as you facilitate, where ongoing support was critical, you could add another Target Concept such as ‘learning is a lifetime thing”. We did toy with this, but being metric, stayed at 10.
All the best
David
David – I mulled over this further and sort of got my head around it. By chance I’ve been sorting some papers and came across a blog post written by Lorimer on the question of ‘Is chronic pain a disease?’ In it he states that the changes that happen in the nervous and other systems (e.g. immune) contribute to pain but they are not sufficient to cause pain. Something I’ve heard him say often. Reviewing this statement again has helped me to understand what you are saying a little better.
So mulling this over further… pain is the normal response to these changes that ramp up the danger signal plus the other factors that make pain the emergent property it is. So it’s not pain that is ‘the disease’ or the ‘abnormal’ experience. The experience of pain emerges from it.
I’m still having a few issues getting my head around how pain can therefore be ‘over protective’.
I suppose what people are doing is calling the combination of central sensitisation, cortical reorganisation, immune involvement etc, chronic pain and I can see how this has happened. Perhaps we need a separate label for this process?
Hope I’m getting there slowly!!
I really like the 10 Target Concepts. They summarize nicely the principles we try to put across with our patients, and would make a great poster for our clinic. I would want to modify the language a bit, as we deal solely with pediatric patients, so it has to be accessible for children and youth, and their parents.
Thanks Allen,
Keep in touch.
We are very interested in how these relate to youngsters. Some researchers have already shown interest. The language will need some changes and perhaps some can be removed and new ones added. We really stress that they are adaptable – last week I added ‘knowledge of the growth spurt provides understanding and direction’ to the Target Concepts used for a teenager with persistent pain.
Cheers
David
Nice work Mr Butler (and Mr Moseley)! The 10 points are all relevant and appropriate for pain management treatment and always nice to have a checklist to cover with patients. My clinical experience is that many concepts in Explain Pain needed to be simplified and clarified for my clients, so I look forward to reading EP supercharged. A point of interest – a few of our clients at the Complex Injury Group have had the experience of going to a physio who has done traditional hands on work, and then given the a copy of EP to read. Understandably, they haven’t really got the concepts.
Right on Edwina,
We regularly hear “I was given a copy of Explain Pain” to read along with various manual therapy treatments. It will rarely work , especially if the manual therapy is sending an alternative message. I also admit we were slow adding the conceptual change strategies to the material but I humbly think we are getting there now.
Best wishes
David
I think these concepts are inter-linked. It is really hard to think that we exclusively use one of them to deal with an individual condition. Even placebo now can be more understandable.In physiotherapy, motivating thoughts can be influential but the effect is objectively hard to measure. We give a lift up to people at times when they are depressed, of course they feel better and they may move easily but what about the possibility of measuring placebo in physiotherapy as an independent intervention. We need really to validate the placebo response so it can be more clinically understood.
Another point about unsmudging technique, what about saying: pain map can be unsmudged. Just a thought.
Thank you,
Ahmad
David, may I direct your attention to Target Concept #1 – “Pain is normal, personal and always real.”?
Would you please define “normal”?
Have you read the paper by Ruth Cronje and Owen Williamson – Is pain ever “normal” ? They suggested that the word “normal” be expunged from the IASP, pain terminology. Their argument was a particularly cogent one.
Reference: https://www.ncbi.nlm.nih.gov/pubmed/16988565
John and Betsan – in this context we use normal as usual, ordinary, natural, fundamental. I like natural. The Williamson/Cronje argument relates to a different context such as how to you measure normal and issues with the so called realness of pain. So for me it is not as the urban dictionary defines “normal” – as “a word made up by this corrupt society so they can single out and attack those who are different”.
Users of this target concept (pain is normal, personal and always real) in an Explain Pain curriculum are offered other suggestions to the wording of the concept such as “your pain is yours, real and unique”, “pain is never imagined”, “if you feel pain you have pain”, “noone else decides whether you are in pain or not” or just plain ”pain is normal” , “pain is natural” or “pain is real”
Target concepts are not commandments as has been commented on social media – they are concepts which when grasped allow a progressive functional knowledge. They are malleable for learner and deliverer.
My patient smiled last week – “mate” I said “with those last two back operations failing, that specialist saying there is no more he can do, the physio given up, you worried about those new leg pains and gut aches, the missus pissed off with you and you worried about your recent high PSA result, its no wonder you need to lift your protection level and having more pain is one of the best ways to increase body protection. In fact it is a normal, natural response and i would think it a bit abnormal if there wasn’t an increase in pain”.
Cheers
David
Can you please let us know when Explain Pain Supercharged is available as an Ebook on Google Play. Very much looking forward,
Thanks for your wonderful resources!!
Hi, can you please give an example of what the target concepts may be for psychological topics presented at a pain group? These topics include awareness of stress, unhelpful thoughts, depression, frustration/anger… Thankyou.
David and Lorimer are legends in my book and I love learning more about these concepts and sharing them with my patients as well as colleagues. Keep up the great work and I will keep sharing your great work while of course giving you guys proper credit!
Cheers!
Ryan Crandall