Professor Michel Coppieters is teaching Mobilisation of the Nervous System in Sydney on July 29-30. Here’s Michel’s post on the sural nerve (one of the most popular ever on NOIjam) to get you thinking neurodynamically.
The sural nerve is a somewhat underrated nerve – most people are taught that it is a sensory branch that innervates the lower postero-lateral part of the leg and the lateral side of the foot. The fact that it is the most common donor nerve for an autologous graft might be mentioned as an aside – suggesting that just like an appendix, one can live happily without it (if not too bothered by a partially numb foot). Although the sural nerve and appendix might not be essential for life, both structures can have significant clinical relevance.
Clinically significant
Only a few days after we published a study on the neurodynamics of the sural nerve, a colleague from Norway shared the story of an elite runner with posterior ankle pain. The runner’s pain had started 2 months earlier when he had slipped on an icy road while training. Reported as initially nothing more than a “stretch”, it gradually became more painful. The pain, about a 4/10 while running, was located above his lateral malleolus and over his Achilles tendon. The pain was reported as becoming more diffuse while running, and more intense with squatting and dorsiflexion. Calf stretches, massage, and a week of no running and NSAIDs, had made little difference.
Achilles tendinopathy, peroneus muscle dysfunction, a fatigue fracture and perhaps anterior impingement might come to mind, but the sural nerve, that underrated sensory branch, also runs in close proximity [Fig 1: Anatomy picture]. Further examination revealed over-pronation of his foot, mild patella tilting, poor hip control during unilateral leg stance and corresponding hip muscle weakness. Assessment of the Achilles tendon and peroneal muscles did not reveal abnormalities, but a modified SLR for the sural nerve and palpation of the sural nerve reproduced his symptoms.
A review of the anatomy
The main sural nerve is a continuation of the tibial nerve, travelling distally between the heads of the gastrocnemius. Near the lower limit of the gastrocnemius, the sural nerve becomes subcutaneous and is joined by a communicating branch of the common fibular nerve (although this is variable).

The sural nerve then runs lateral to the Achilles tendon, behind the lateral malleolus and along the lateral border of the foot:

Sural nerve pathology can be caused by internal factors, such as compression due to fascial thickening, increased calf muscle mass, local scar tissue, mass-lesions (tumours), haemorrhage or abscess, or external factors, such as tight ski-boots, casts or tight footwear. Injury to the sural nerve can occur from an inversion ankle sprain, fracture of direct blow.
The neurodynamics of the sural nerve
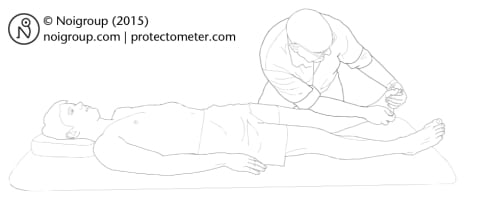
The neurodynamic test for the sural nerve (SLRSURAL) is similar to other lower limb neurodynamic tests, but specificity for the sural nerve is added with foot positioning and order of movement. For SLRSURAL, the ankle and foot are first moved into dorsiflexion and inversion to load the dorsolateral ankle and foot structures, including the sural nerve:
Hip flexion is then added as a sensitising manoeuvre:
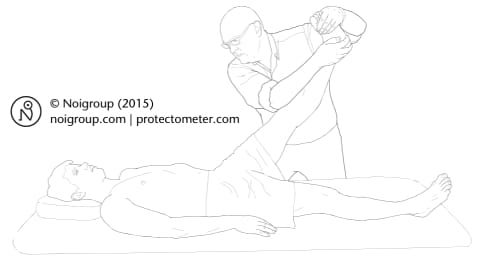
With the foot and ankle positioning maintained:

The biomechanical rationale for this procedure is that once the dorsolateral ankle and foot structures are placed under load by initial positioning of the foot, strain in the sural nerve can be selectively and somewhat exclusively increased with the addition of hip flexion. Reproduction or modulation of symptoms with hip flexion suggests sural nerve (or perhaps more broadly, nervous system) involvement.
Although there is little research on the reliability or validity of any clinical test for the sural nerve currently, our recently published article (linked above) demonstrated that hip flexion did increase the strain in the sural nerve in cadaveric specimens, providing biomechanical support for the SLRSURAL.
Back to the runner in the clinic
Based on the neurodynamic findings, management was quite straightforward. The patient was educated about the problem and what could be done about – including what he could do himself. Neurodynamic mobilisation of the sural nerve was undertaken with a home program provided. Some hip and balance exercises were prescribed to address other issues picked up during examination. The patient was seen on four occasions. He is training happily again and is looking forward to the Norwegian athletics championships.
Although the exact pathomechanism is often difficult to determine, being more aware of this ‘forgotten’ nerve and considering neurodynamics as part of a rehabilitation program may bring some relief to runners (and others) with persistent posterior-lateral ankle pain.
– Terje Skulstad
Useful Links
Bodily Relearning, Boyd BS
Neurodynamic techniques Handbook & Videos, Butler DS
The Sensitive Nervous System, Butler DS
Nice one Michel and Terje,
This is surely a missed nerve in foot pain. I have known a number of people with lateral ankle “impingements” where clinicians have been playing around with foot biomechanics yet in the test described above similar pains in the foot were easily provoked by hip flexion.
David
Interesting post
Interesting. Good clinical knowledge. Thanks for sharing!
Great write up, I’ve been dealing with idiopathic medial foot pain for 13 years, see the world famous Dr. Dellon soon. Do you guys have any resources for Tibial or Calcaneal (or any medial/heel) nerve pathologies?