
In this world of brain plasticity and the excitement it engenders, we may sometimes forget the complexities of the rest of the body and maybe also, the rest of the nervous system.
The T6 area in the clinic
What is it about the T6ish area? The middle of the back is a very popular place to experience pain and tightness. About 30 years ago, as neurodynamics thinking emerged, I was intrigued with this area. A repeated clinical pattern exists where many people with positive straight leg raises (SLR) or slump tests often complain of pain around the T6 area. Additionally, if someone had a positive SLR or passive neck flexion, suggesting some alteration of meningeal biomechanics, palpation around the T6 area often revealed tenderness and stiffness, usually unbeknown to the owner of the back. People, post whiplash, often have this finding and indeed whiplash sufferers who complain of pain in the mid thorax may have a worse prognosis (Maimaris, Barnes et al. 1988). Many clinicians reading this blog are well aware that if you gave the mid-thorax a bit of a wriggle and shake, the whole body movement can improve and SLR and slump test findings will often improve, sometimes markedly.
The science
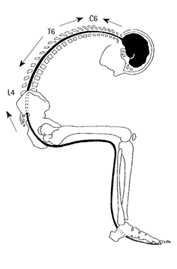
Intriguingly, some science on neuromeningeal biomechanics emerged at the time of developing neurodynamic theories. With an extrapolation from a 24 human cadaver study by Louis (1981), supported by earlier work by Breig (1978) and painstaking monkey dissections by Smith (1956), the year I was born! I came up with the image below from “Mobilisation of the Nervous System (1991). The spinal canal could be around 9 centimetres longer in flexion than extension – somehow the contained cord and meninges have to adapt. Check out the T6 area – it doesn’t move that much in relation to the surrounding canal – kind of like if you pull a piece of elastic from both ends, there is a bit in the middle that doesn’t move much in relation to its surrounds.
If there was something special about the area then you would expect that the anatomy would express something about the function. While there has been minimal study (and few would bother today), the major blood vessel for the thoracic cord and meninges comes in just under T6 – so it’s probably not a good place to have a lot of sliding around, and in addition, the canal here is quite narrow and the dura mater is thicker than anywhere else along the neuraxis. Maybe it is designed to be like the middle of a piece of elastic?
T6 today
Pause a moment and marvel– the spinal cord in the thorax may only be a little over a centimetre in diameter with the surrounding canal maybe around 1.4 centimetres and also containing meninges and cerebrospinal fluid (CSF) whose freshness is necessary for cord nutrition. This tiny area has a lot of work to do in representing the low back, pelvis and legs. I think it is best to add the cord into modern concepts of representation and neuromatrix which are often all brain based.
I think that no matter what, if central sensitisation is considered, then the physical health of the nervous system including the cord should be entertained. Is the T6 area a place that is perhaps biomechanically more at risk than other parts of the nervous system especially when you consider what humans do with their bodies these days? Physical problems with physiological consequences could result in significant nociception from the meninges, peripheral neurogenic contributions from sinuvertebral nerves innervating the meninges, and nerve roots plus mechanically induced contributions to sensitisation. The slump test, especially in long sitting may be useful to check it out and I am sure the area loves inputs such as yoga, dance, martial arts and just a good old roll around on the floor.
In conclusion, there is a place in the biopsychosocial framework for T6.
Tell us your T6 stories
–David Butler
– Breig, A. (1978). Adverse Mechanical Tension in the Central Nervous System. Stockholm, Almqvist and Wiksell.
– Louis, R. (1981). “Vertebroradicular and vertebromedullar dynamics.” Anatomia Clinica 3: 1-11.
– Maimaris, C., M. R. Barnes, et al. (1988). “‘Whiplash injuries’ of the neck: a retrospective study.” Injury 19: 393-396.
– Smith, C. G. (1956). “Changes in length and position of the segments of the spinal cord with changes in posture in the monkey.” Radiology 66: 259-265.
Related reading
Bodily Relearning, Boyd BS
Neurodynamic techniques Handbook & Videos, Butler DS
The Sensitive Nervous System, Butler DS
The neurobiomechanics of that area has always confused me. It doesn’t move in the classic slump where both ends of the neural axis move at the same time, but how much movement is there when one end is off tension and the other is now placed on tension, essentially caudal or cranial directed glides? Does this have any relation to the infamous T4 syndrome? Johnb
Hi John,
I guess noone really knows – but maybe not much – best to move the meningeal cord apparatus where there is a bit more canal space and no arteries coming in. I think this area is perhaps a bit vulnerable when we consider what humans do it – such as sitting and growing old.
Ah – T4 syndrome – It is infamous! I wish it would roll over and die! – Here we have sometime complex pain states reduced to a one bone label! Maybe the postulated vulnerabilty of the T6 area helped create the “T4 syndrome” with some manual therapists not counting spinous processes so well?
Best wishes
David
Whilst reading this article I was visited by my old friend ” Central chest pain” which is nasty in nature, using Geoff Maitlands terminology……..A roll on the floor and a click at T6 works wonders…….Taken as a model for demonstrations during practical lectures back in 1978 by Geoff personally he commented on his palpation findings of my T6 area. Following a grade give triple plus P/A thrust Geoff commented on the nasty type of chest pain problems in this area could produce ………..food for thought ………