
“Play is often talked about as if it were a relief from serious learning. But for children play is serious learning. Play is really the work of childhood.”
– Fred Rogers
Children seem to have endless energy and spend their days playing and pretending – kicking balls, riding bikes, fighting dragons, twirling through pretend snow singing Elsa’s ‘Let it go’. Play is an essential part of childhood. But just like adults, when children experience persistent pain they too develop fear of movement. It hurts and so they move less, they play less.
Gone are the days where the mainstay treatment for pain was rest – especially for chronic pain. Now we educate, we talk and we explore graded exposure to movement. But one of the barriers we come up against is this inherent fear of performing a movement that hurts. Fear of movement is a driving force that impedes treatment progress. So to be effective, we need to identify and prioritise movement-related fears and find ways to discuss and address them.
In 2017 a research team at Boston Children’s Hospital and Stanford University helped start us off by creating an electronic tool to identify and prioritise worry and anticipated pain in children. It’s called the PHODA-YE, or the Photographs of Daily Activities for Youth in English. The original PHODA was made for adults and introduced in 2007, later adapted to be used for Dutch children in 2015.
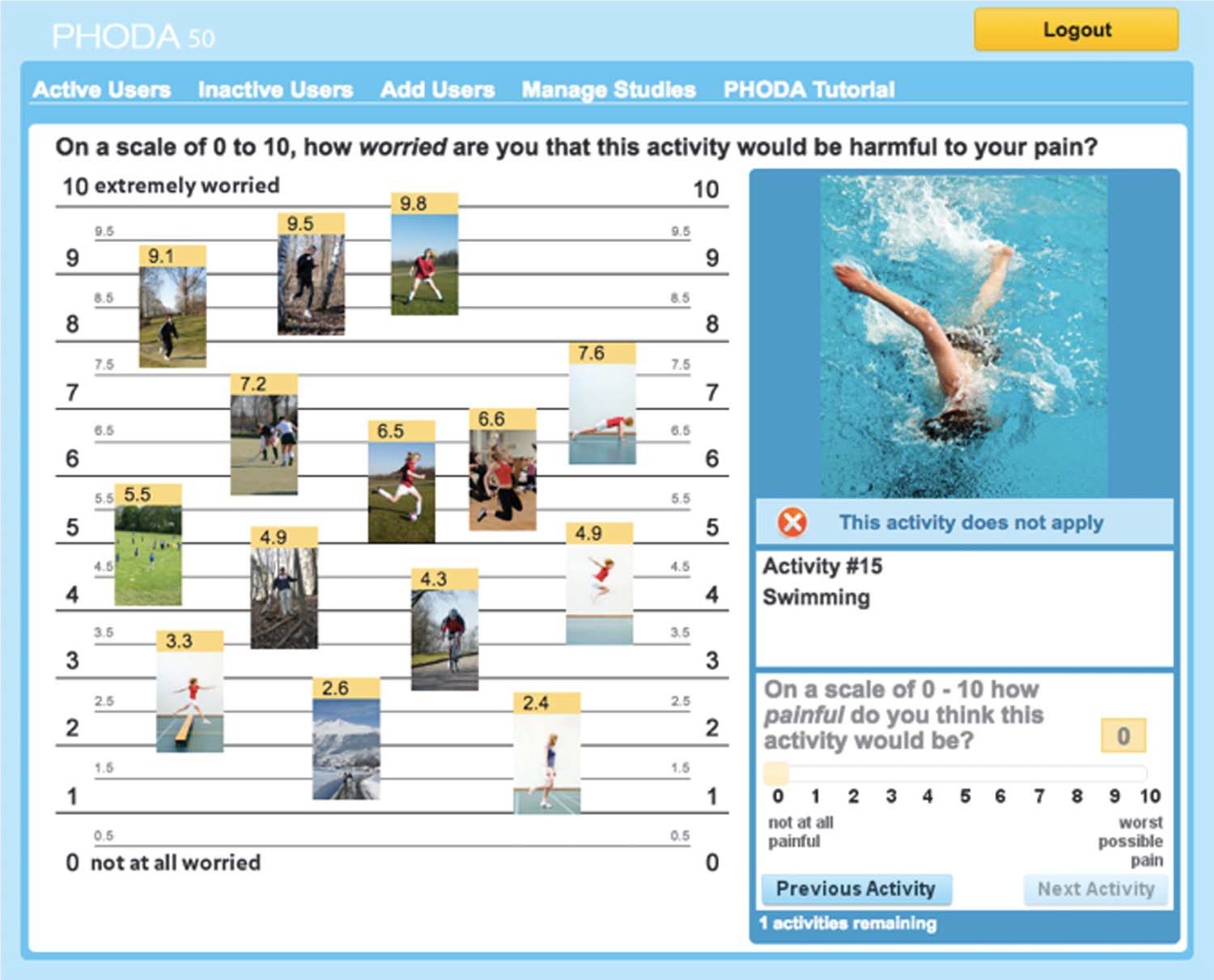
This is how it works. The child sits down at a desktop computer or a tablet. They read some basic instructions and are then shown 2 mock images in a tutorial. The assessment begins. For each of the 50 photograph the child is asked “On a scale of 0 to 10, how worried are you that this activity would be harmful to your pain?”. To answer they drag and drop the picture on a worry scale ranging from 0 (not at all worried) to 10 (extremely worried). Next, the child is asked, “On a scale of 0 to 10 how painful do you think this activity would be?” and they slide a bar between anchors of 0 and 10. They can skip the activities that don’t apply to them. In total it should take about 30 minutes and at the end, the clinician is provided a report of the findings.
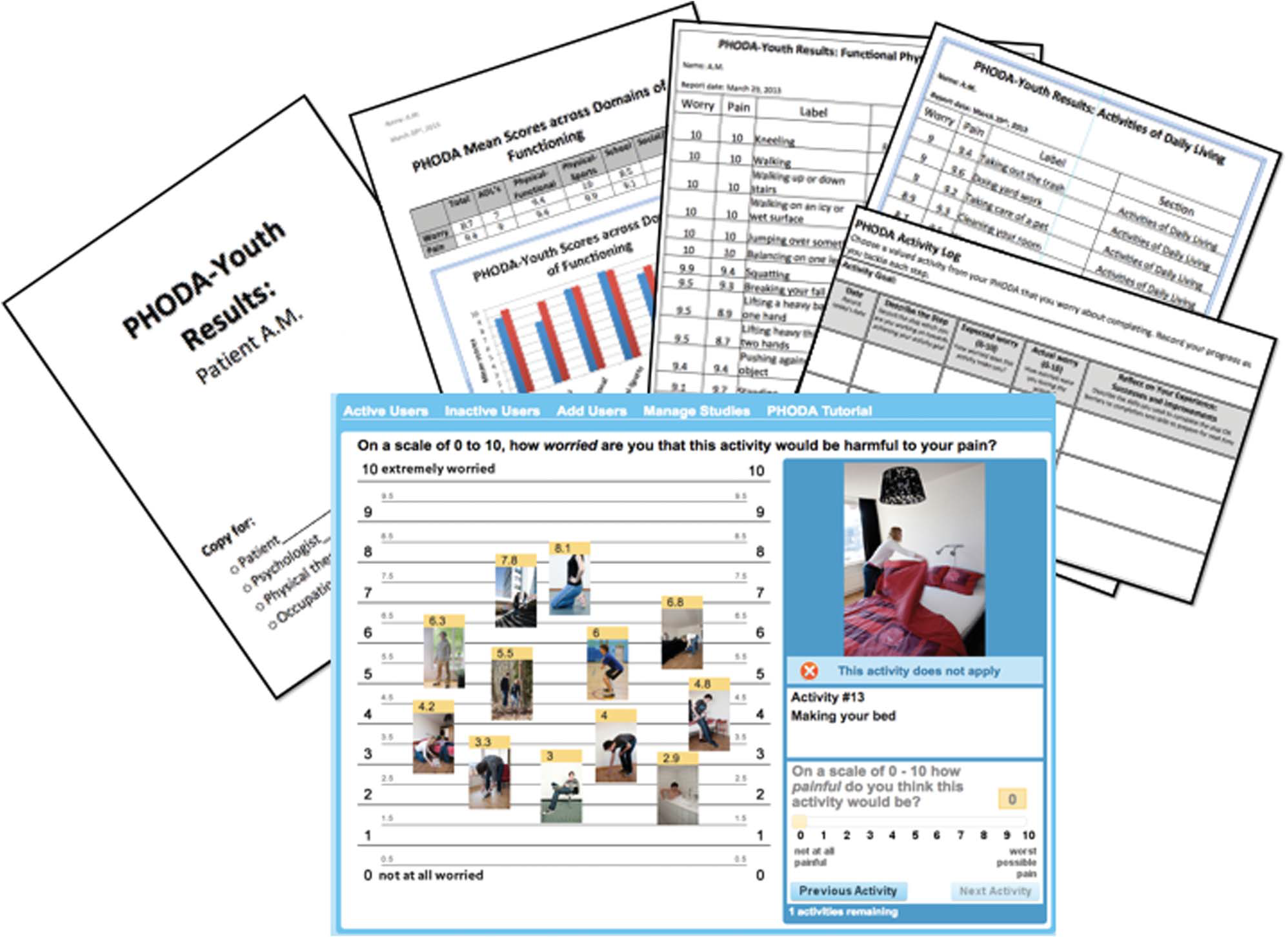
The study that introduced the English version for children found the tool to be psychometrically sound and valid. The creators recommend multiple providers (eg. psychology, PT, and OT) discuss the results with the child and their family/carers and integrate identified worrisome activities into graded exposure treatment.
If you or your institution are potentially interested in implementing the PHODA-YE in your clinic or to use it for research, please contact Laura Simons at [email protected].
– Hayley Leake
comments