Uncertainty is everywhere in clinical practice. For those seeking help, uncertainty may emerge from unfamiliar or unpredictable symptoms, persisting pain, or confusion about what treatments are best, what the future holds, and who to trust. For clinicians, uncertainty arises in how we build therapeutic relationships, the accuracy and utility of our assessments, the choice and application of treatment, and even in our own knowledge (Costa et al. 2022).
Uncertainty can feel uncomfortable – sometimes even threatening – and both clinicians and patients often respond by trying to eliminate or avoid it. Yet, as emerging theoretical frameworks suggest, leaning into uncertainty can be a critical strategy for reducing it over time, enabling us to become better equipped to navigate future challenges (Kilverstein et al. 2019).
A growing body of literature highlights the value of tolerating uncertainty. For clinicians, this tolerance is associated with reduced burnout, improved job satisfaction, better engagement with patients, and a greater likelihood of guideline-concordant care – with less overuse of unnecessary tests and treatments (1–4). For patients, greater uncertainty tolerance is linked to improved trust in healthcare providers, reduced healthcare utilisation, and a stronger capacity to manage ongoing challenges (Stephens & Lazarus, 2024). This suggests that supporting both clinician and patient tolerance of uncertainty may be a meaningful target in clinical care.
Of course, there are aspects of clinical work where we should strive for certainty. Recognising and responding to red flags or medical emergencies is essential, and confidence in our ability to detect serious pathology matters – even if uncertainty remains part of that picture. Likewise, when diagnostic testing has strong reliability and treatment pathways are well-established, such as in type 2 diabetes, certainty is clinically beneficial. But, in pain care, these conditions of diagnostic clarity and predictable treatment response are less common. The inherently subjective and multifactorial nature of pain adds layers of complexity to our clinical interactions.
So, what practical ways might we support tolerance of uncertainty, for ourselves and those we care for?
- Consider how we establish safety. Safety can be cultivated through active listening, validation of the person’s experience, thorough assessment, and a strong therapeutic alliance.
- Reframe uncertainty as a context for learning and adaptation. This shift in mindset may create more space for exploration.
- Reflect on your own relationship with uncertainty. Can you sit with it? Is it safe to do so? This reflection may also help clarify when to involve a broader, multidisciplinary team.
- Consider the person’s current capacity. Do they have the safety and support needed to engage with uncertainty right now?
- Reflect on identity in care: can we become facilitators (rather than fixers), supporting their own process of exploration?
One strategy we might consider is play. Here, we’re defining play as exploration driven by curiosity, flexibility, and intrinsic interest (Andersen et al., 2022). Play invites exploration without fear of failure, fosters adaptation through experience, and makes room for surprise – an essential ingredient for learning. When something unexpected happens in a safe context, the system has an opportunity to adjust and adapt. In clinical practice, this might mean designing tasks or environments that invite patients to explore and problem-solve within novel yet manageable challenges.
But there’s a balance to strike. Too much uncertainty is overwhelming and disengaging. Too little, and people may simply reinforce old, unhelpful beliefs – that their body is fragile or their condition irreversible. The Sweet Zone lies in the middle: enough uncertainty to challenge but not so much as to be highly threatening (See Fig 1). In this space, people can safely test assumptions, gather evidence of change, and build more flexible, empowered models of themselves. The Sweet Zone isn’t static – it shifts with context, mood, confidence, and support – and as uncertainty is gradually reduced, the challenge must evolve to maintain that edge of learning.
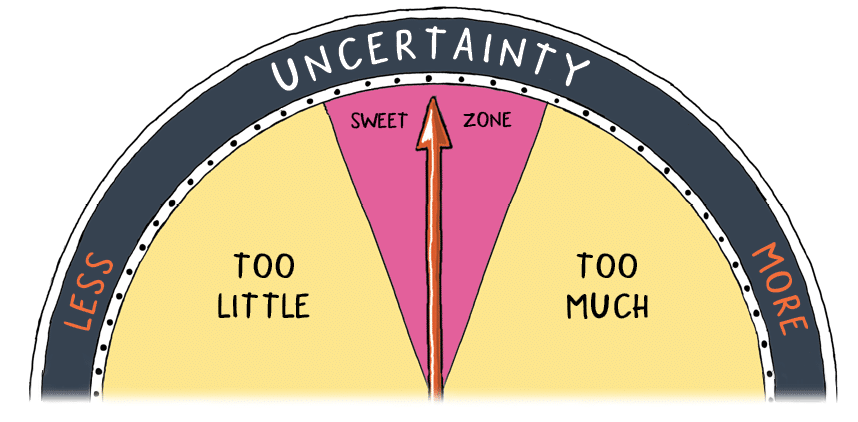
Fig 1. The Sweet Zone of Uncertainty. Adapted from the Resolve Back Pain Handbook. Noigroup Publications. 2024.
Uncertainty is often seen as something negative – something to eliminate. But on closer inspection, it is also an opportunity: an opportunity for discovery, for change, for growth. Helping someone successfully navigate uncertain situations may allow them to experience meaningful surprise, reinforce a more adaptive understanding of their body and their capacity, and build self-efficacy through action. As Miller et al. (2019) explore in their paper titled, Embodying affective intentionality: towards a theory of affective skill, how quickly or slowly we resolve uncertainty compared to our expectations can shape our emotional experience and our future motivation, i.e., when we resolve uncertainty faster than expected and successfully, it feels good. In clinical care, setting someone up to successfully engage with – and resolve – manageable uncertainty may be a powerful lever for recovery – feeling deeply rewarding and motivating.
Our education systems often train us to seek certainty, to find the right answer, and to avoid ambiguity. But if we can learn to work with uncertainty – to accept it, reflect on it, be open to others about our own uncertainty, and use it to support learning – then we not only enhance our clinical practice but better support the people who come to us for help.
What uncertainty are you carrying that – if shared/embraced – might create space for growth, connection, or change?
– Brendan Mouatt, CEO Noigroup
References
- Begin, A. S., Hidrue, M., Lehrhoff, S., Del Carmen, M. G., Armstrong, K., & Wasfy, J. H. (2022). Factors associated with physician tolerance of uncertainty: an observational study. Journal of General Internal Medicine, 37(6), 1415–1421.
- Begin, A. S., Hidrue, M. K., Lehrhoff, S., Lennes, I. T., Armstrong, K., Weilburg, J. B., … & Wasfy, J. H. (2022). Association of self-reported primary care physician tolerance for uncertainty with variations in resource use and patient experience. JAMA Network Open, 5(9), e2229521.
- Ghosh, A.K. (2004). Understanding medical uncertainty: a primer for physicians. Journal of Laboratory and Clinical Medicine, 144(2), 60–64.
- Allison, J.J., Kiefe, C.I., Cook, E.F., Gerrity, M.S., & Orav, E.J. (1998). The association of physician attitudes about uncertainty and risk taking with resource use in a Medicare HMO. Medical Decision Making, 18(3), 320–329.
- Stephens, T., & Lazarus, M.D. (2024). Twelve tips for developing healthcare learners’ uncertainty tolerance. Medical Teacher, 46(2), 1–6.
- Miller, M., Kiverstein, J., & Rietveld, E. (2019). Embodying affective intentionality: towards a theory of affective skill. Topoi, 38, 175–189.
- Costa, N., O’Sullivan, K., O’Sullivan, P.B., et al. (2022). The ubiquity of uncertainty in low back pain care. European Journal of Physiotherapy, 24(3), 142–148.
- Kiverstein, J., Miller, M., & Rietveld, E. (2017). The feeling of grip: Novelty, error dynamics and the predictive brain. Synthese, 1–23.
comments