Published late last year without much fanfare, this paper raises some crucial challenges for the current understanding of, and treatment rationale for, CRPS.
Fine-Grained Mapping of Cortical Somatotopies in Chronic Complex Regional Pain Syndrome
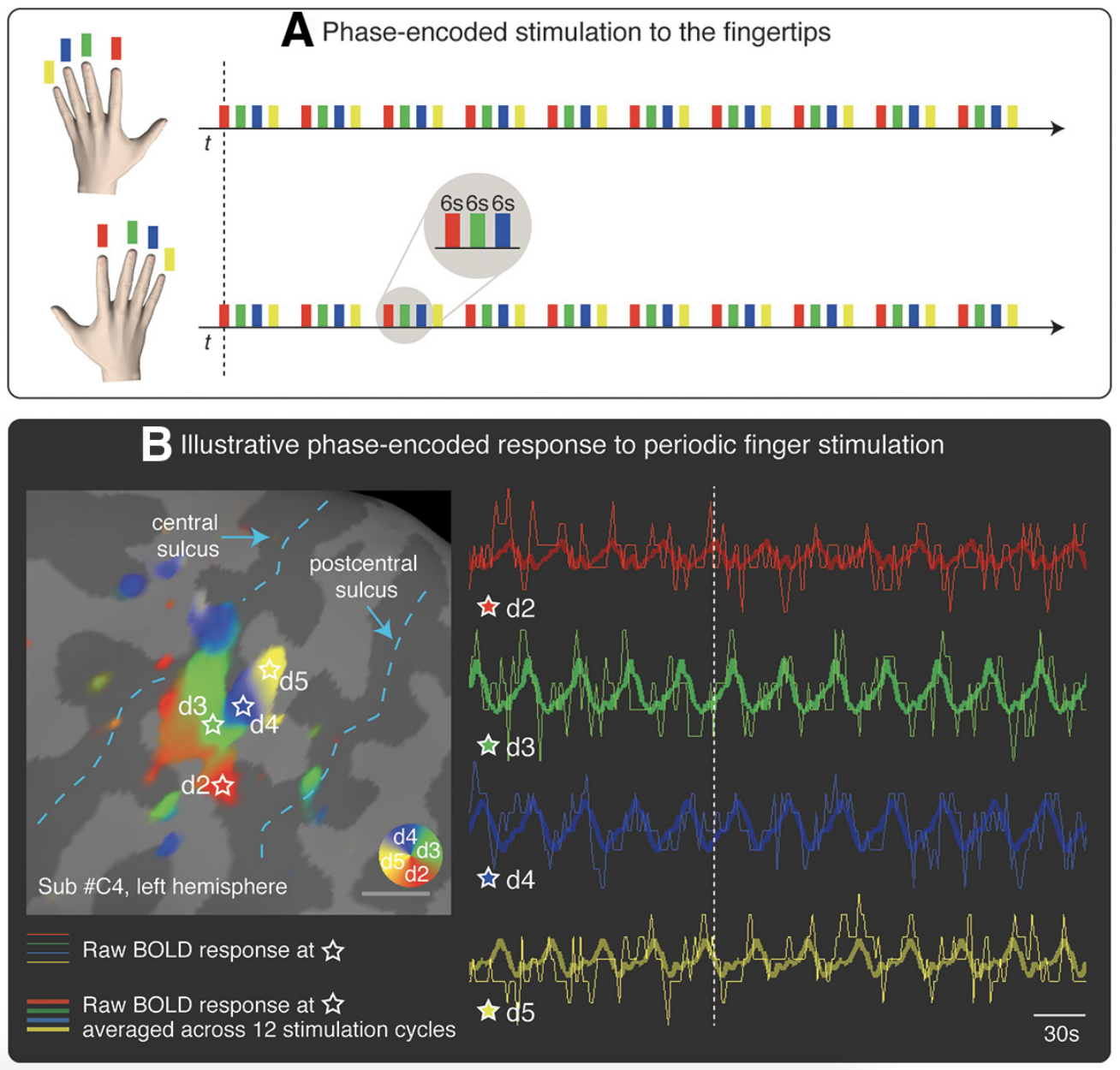
ABSTRACT: It has long been thought that severe chronic pain conditions, such as complex regional pain syndrome (CRPS), are not only associated with, but even maintained by a reorganization of the somatotopic representation of the affected limb in primary somatosensory cortex (S1). This notion has driven treatments that aim to restore S1 representations in CRPS patients, such as sensory discrimination training and mirror therapy. However, this notion is based on both indirect and incomplete evidence obtained with imaging methods with low spatial resolution. Here, we used fMRI to characterize the S1 representation of the affected and unaffected hand in humans (of either sex) with unilateral CRPS. The cortical area, location, and geometry of the S1 representation of the CRPS hand were largely comparable with those of both the unaffected hand and healthy controls. We found no differential relation between affected versus unaffected hand map measures and clinical measures (pain severity, upper limb disability, disease duration). Thus, if any map reorganization occurs, it does not appear to be directly related to pain and disease severity. These findings compel us to reconsider the cortical mechanisms underlying CRPS and the rationale for interventions that aim to “restore” somatotopic representations to treat pain.
SIGNIFICANCE STATEMENT This study shows that the spatial map of the fingers in somatosensory cortex is largely preserved in chronic complex regional pain syndrome (CRPS). These findings challenge the treatment rationale for restoring somatotopic representations in complex regional pain syndrome patients.
From the discussion
We show that the cortical map of the fingertips of the CRPS hand in S1 is strikingly comparable with the map of the unaffected hand and controls in terms of area, location, orientation, and geometry. Our results do not exclude that other abnormalities may occur at S1 level, such as excitability changes (Lenz et al., 2011; Di Pietro et al., 2013), morphological (Baliki et al., 2011; Pleger et al., 2014; compare van Velzen et al., 2016), and connectivity changes (Geha et al., 2008). However, our findings challenge or, at the very least, narrow the notion of S1 map reorganization in CRPS. Thus, even if a map reorganization occurs, it does not appear to be directly related to pain severity and upper limb disability.
These findings urge us to reconsider the mechanisms that are currently proposed to underpin CRPS (Marinus et al., 2011). They also compel us to reevaluate the rationale for clinical interventions that aim to reduce pain by “restoring” somatotopic representations with sensory discrimination training (Moseley et al., 2008b; Catley et al., 2014), or by correcting sensorimotor incongruences (which are thought to be induced by S1 reorganization) with mirror therapy (McCabe et al., 2003; but see Moseley and Gandevia, 2005; Moseley et al., 2008b). Although these interventions appear to offer clinical benefit (O’Connell et al., 2013), they are unlikely to engender a “restoration” of somatotopic representations in S1, which are largely comparable to those of controls. (emphasis added)
These are striking findings with strong conclusions. They raise some important, challenging and potentially uncomfortable questions for those of us involved in the promotion and teaching of strategies for the treatment of CRPS. The findings warn against thinking that is reductionist and simplistic, too ‘brain-centric’ in relation to a condition that is, as it says right there on the tin, complex. A rethink, at the very least on explanations of mechanism, is on the cards.
The full paper is available open access here.
Discussion and thoughts welcome below.
-Tim Cocks
Review further noijam blogs on CRPS
Find out more about the Graded Motor Imagery process and GMI resources.
Maybe we haven’t completely figured out the workings but outcomes suggest we are on the right track so let’s not throw out the baby with the bath water 🤔
Completely agree
Yes this paper stumped and surprised me and I was a little shocked at the lack of fanfare.
I don’t fully understand fMRI studies and certainly don’t claim to have even a basic grasp of pain neurophysiology, but I do spend a lot of my time thinking about how the brain works and all of my professional time treating patients with chronic pain.
One thing I do know is that GMI works. (At least it’s does in the kids I treat). When I came across this paper The first thing I thought of was – ‘but There must be changes in the somatosensory cortex because we have to work so hard at the visualisation stage with kids because their imagination is so profound’. If we don’t change the thoughts and feelings about those visualisations, then we know they don’t get better. Then it hit me – it’s not represented in the somatosensory cortex alone. It might be the neurotag size and weight attached to each portion of the somatosensory cortex (ie. the thoughts, feelings, memories associated with the hand) and then how does the brain perceive the size and weight of that neurotag as credible evidence to protect??
Measure that with fMRI
I have followed the work of Flor and Loz for many years and it made sense and loves it. With advances in fMRI and problems with the accuracy of the algorithms where does this leave the evidence with regards to cortical reorganization in amputees and also smudging in chronic pain patients?